Healthcare reform has become not only a landmark example of ongoing transformations in the mindset of Ukrainians – it has, in many ways, become synonymous with the very “reform” concept.
This article examines what has been achieved and what remains to be accomplished in the transformation of Ukrainian hospitals, as well as how society perceives this large-scale initiative aimed at overhauling the entire healthcare system.
The transformation of Ukraine’s healthcare system began in October 2017 with the adoption of the Law of Ukraine “On State Financial Guarantees of Medical Services to the Population” (No. 2168-VIII).
The primary objective of this law was to move away from the outdated Soviet-era model, commonly referred to as the “Semashko” system, which was characterised by centralised state control, rigid administrative oversight, and financing based on the number of hospital beds. Instead, the reform sought to align Ukraine’s healthcare system with more efficient models of universal health coverage, focusing on delivering services based on actual needs rather than institutional capacity.
The healthcare reform in Ukraine is being implemented in three distinct phases:
The first phase of the reform is generally considered fully implemented. Over 30.91 million declarations have been submitted by patients selecting their primary care physicians.
As part of this stage, the National Health Service of Ukraine (NHSU) was established, and a unified electronic healthcare system was launched.
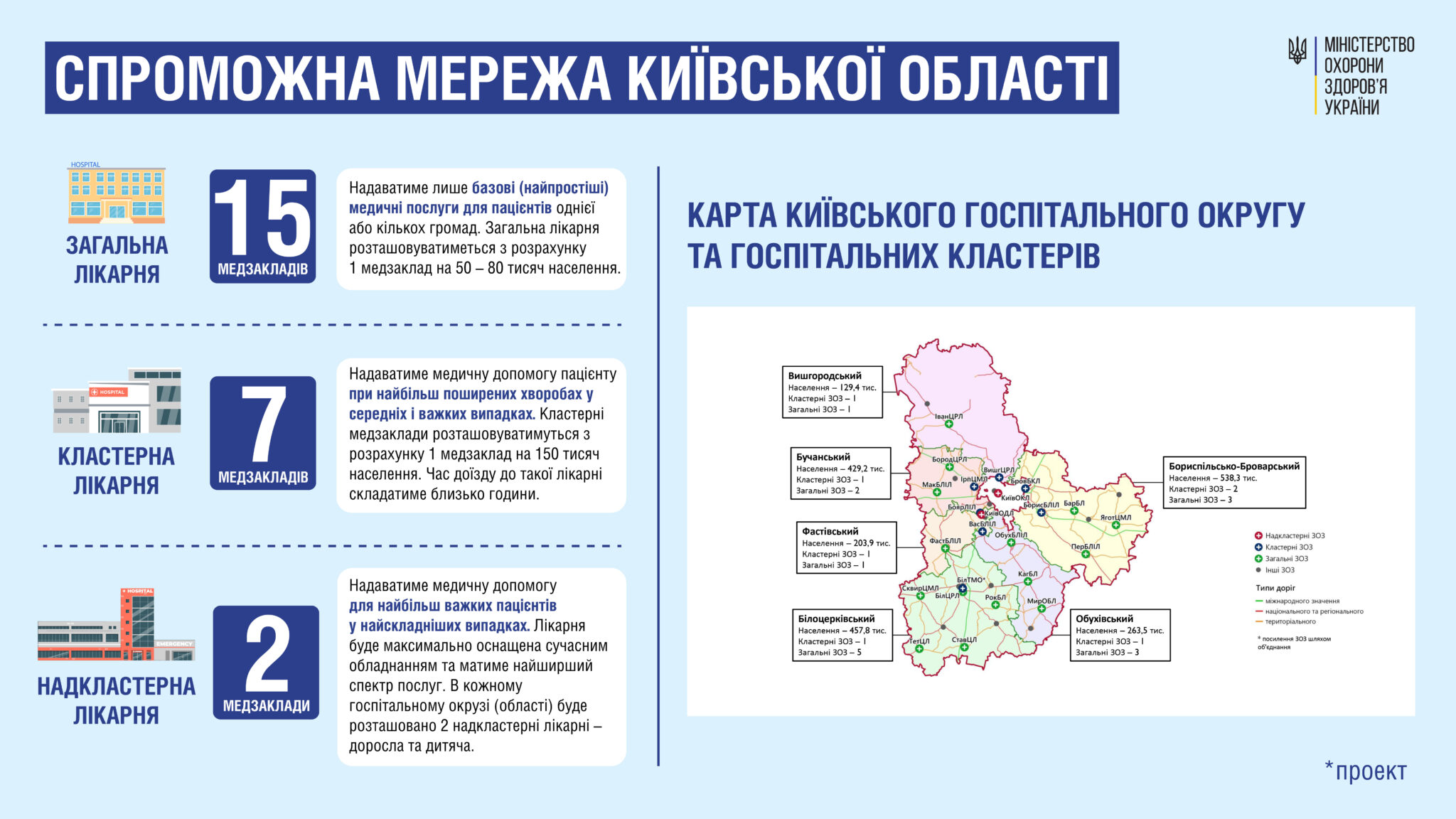
The second phase remains in implementation. Despite the full-scale war, the Ukrainian state has maintained its commitment to healthcare reform. In 2022, the Verkhovna Rada adopted a law aimed at improving the provision of medical care. This law formally merged the concepts of secondary and tertiary levels of healthcare, laying the regulatory groundwork for the establishment of hospital districts and their classification into the aforementioned clusters.
In 2023, the Cabinet of Ministers adopted a resolution that defined the operational mechanisms for these clusters. At least on paper, hospitals received financial autonomy and access to new funding sources. Healthcare facilities are being organised into corresponding hospital districts – excluding those in temporarily occupied or frontline territories.
The third phase has only recently begun. As of January 1, 2025, all state-owned healthcare institutions have started integrating into the unified medical space and the Program of Medical Guarantees.
This process includes explicitly institutions under the National Academy of Sciences, the National Academy of Medical Sciences, and the State Management of Affairs.
After eight years of development, Ukraine’s healthcare reform has only recently entered its third phase. Nevertheless, these decisions indicate a continued – if cautious – commitment by the Ministry of Health not to shelve the reform altogether. International organisations have responded positively to the progress achieved thus far. According to a joint report by the World Health Organization (WHO) and the World Bank, the overall structure of Ukraine’s healthcare financing reform aligns with leading global practices aimed at improving access, quality, and efficiency in medical service delivery. Their earlier assessments also noted that the National Health Service of Ukraine (NHSU) had achieved tangible results in primary care during its initial years of operation. It is widely acknowledged that, despite the war, Ukraine has managed to preserve universal healthcare coverage under the Program of Medical Guarantees.
1. Reforms in Primary Healthcare (PHC)
One of the most pressing areas for reform is primary healthcare. Current legislation treats PHC as a distinct segment, separate from other levels of care, such as specialised services. To ensure that PHC remains accessible, efficient, and cost-effective, amendments to the relevant legal framework are needed. This includes clarifying the responsibilities related to monitoring and providing access to services. This need is especially evident given that the first phase of the healthcare reform – focused on PHC – is considered the most fully implemented.
Another challenge is the exclusion of private clinics from the official PHC network. This fragmentation of the system may result in uneven service quality for patients. Contributing factors include the current regulatory environment governing licensing, hospital accreditation, and the legal treatment of medical errors, as well as the tort liability of healthcare institutions and practitioners.
The WHO has recommended modifying the PHC service procurement model. Specifically, it suggests integrating small practices into the rural healthcare network and encouraging the creation of group practices in more populated regions. These proposals are based on the recognition that small clinics cannot often provide the full range of services covered by the per capita financing model and face challenges in hiring qualified staff.
Although the number of PHC doctors has increased, many are from diverse specialities and lack unified, generalist training. Additionally, Ukraine faces a severe shortage of nursing staff. The current nurse-to-doctor ratio is approximately 1:1, whereas in developed countries, this ratio is significantly higher.
There are also no standardised and legally established procedures for:
• assessing patients’ needs for medical services,
• updating the package of guaranteed services,
• reviewing existing services,
• calculating their costs and determining pricing, or
• managing NHSU payments and budget allocation within the Program of Medical Guarantees.
2. Clarifying the Legal Basis for Hospital Clusters
The plan to implement a hospital cluster system also requires more explicit legal definitions and criteria. A significant obstacle in forming an effective hospital network is the coexistence of public and private hospitals under different ownership models. According to the WHO, this has complicated efforts to rationalise the healthcare system. Some hospitals have been designated as “cluster facilities” despite lacking sufficient capacity to handle the patients’ influx. In contrast, facilities with better equipment and greater accessibility were excluded due to differences in ownership structure. As a result, instead of pooling resources and coordinating service provision, hospitals are beginning to duplicate services in an attempt to meet NHSU requirements independently. The initial idea of clusters – as a way to optimise hospital networks – is no longer being implemented as originally intended.
3. Adoption of National Strategies on Innovation and Healthcare Development
Over the past six months, the Cabinet of Ministers of Ukraine has adopted two strategic frameworks that will remain in effect until 2030: one for digital innovation development and another for advancing the healthcare system. These strategies envision the integration of innovative technologies into medical services – such as artificial intelligence, remote patient monitoring, and other advanced tools. In turn, healthcare institutions are expected to be equipped with the necessary instruments to apply these technologies while adhering to ethical standards and regulations. However, whether such long-term strategies are meaningful in a legal environment where laws change almost daily remains an open question. Their adoption must be followed by the development of clear methodological guidelines and explanatory materials for both healthcare providers and patients.
Without effective communication, the reform may once again face setbacks, including gaps in implementation, funding challenges for technology-driven services, and renewed scepticism or resistance to innovation in the healthcare sector.
According to a March 2019 survey conducted by the Razumkov Centre, 65.2% of respondents had a negative view of the healthcare reform. Similarly, a 2020 survey by the Rating Sociological Group found that 64% of Ukrainians were mainly dissatisfied with the reform. As recently as December 2024, a study by the Glavkom Information Agency reported that 54.01% of respondents believed the reform had worsened the situation.
Whether the percentage of dissatisfied citizens will decline in the future remains uncertain. Too many variables influence this outcome – and none diminish the urgent need for clear and coherent legislation.
To meet public demand, the Ministry of Health has announced plans to reduce prices by 30% for the 100 most commonly used medicines produced by Ukrainian manufacturers. It has also launched inspections of hospitals to ensure transparency in drug pricing within pharmacies. As of January 1, 2025, scheduled inspections of pharmacy establishments have resumed.
The state is responding to citizens’ concerns, but restoring public trust in the national healthcare system will require many more years – and significant changes in state policy approaches.
In the future, legal assessments will be required to evaluate the outcomes of the experimental project, which provides expanded primary healthcare services to military personnel. Additionally, the legal implications of repealing the Commercial Code of Ukraine for the operation of healthcare institutions will need to be thoroughly examined.
These are just a few examples among many complex legal issues that continue to shape the trajectory of Ukraine’s healthcare reform.
Can we say that the healthcare reform will ever be completed – at least on a legal level? The question is rhetorical. Even the Minister of Health, Viktor Liashko, acknowledges that “healthcare reform in Ukraine is a continuous process that adapts to current challenges, emerging technologies, demographic shifts, and workforce dynamics” and that “healthcare reform will never truly be finished. Modernisation will always continue.”
Despite the extensive journey of healthcare reform in Ukraine since 2017, its results remain mixed. On the one hand, several positive developments warrant recognition, including the establishment of a unified electronic healthcare system, the introduction of the National Health Service of Ukraine (NHSU), and the transition to a new model of service financing. On the other hand, critiques persist regarding system fragmentation, uncertainty around the integration of medical innovations, and the inability of certain institutions to fulfil the roles assigned to them under the cluster-based model.
During wartime, constant legislative change, the prioritisation of defence spending, the idea of healthcare reform as a permanent and evolving process deserves serious consideration. Still, it is possible to improve public trust in the reform. This could be achieved through the liberalisation of restrictions for the medical business sector and clear, systematic communication – especially via simple and accessible explanatory materials.
Therefore, clarity and consistency in health policy are not merely desirable – they are critically necessary.
No posts found!
© 2026 ALL RIGHTS ARE RESERVED